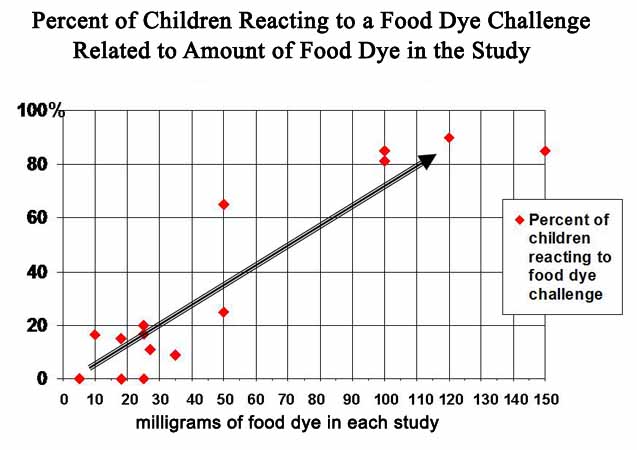
 Critics say that “studies show” that the Feingold Diet helps only 5% (or 2% or 1%) of the children who use it. They generally don’t cite any studies to support this, which is understandable, since there aren’t any. Often, the source cited is a report from a 1982 National Institutes of Health panel which examined the research from the late 1970s through 1981. The panel concluded that while the Feingold Diet is a valid option for the treatment of hyperactivity, the then-existing studies did not support the clinical reports of 60 to 70% success. However, the panel said, the studies were flawed as most of them focused on dyes only, ignoring other aspects of the diet, such as artificial flavors, preservatives and salicylates. “Therefore, these controlled challenge studies do not appear to have addressed adequately the role of diet in hyperactivity.” (See Defined Diets and Childhood Hyperactivity, published by the NIH in 1982).
Critics say that “studies show” that the Feingold Diet helps only 5% (or 2% or 1%) of the children who use it. They generally don’t cite any studies to support this, which is understandable, since there aren’t any. Often, the source cited is a report from a 1982 National Institutes of Health panel which examined the research from the late 1970s through 1981. The panel concluded that while the Feingold Diet is a valid option for the treatment of hyperactivity, the then-existing studies did not support the clinical reports of 60 to 70% success. However, the panel said, the studies were flawed as most of them focused on dyes only, ignoring other aspects of the diet, such as artificial flavors, preservatives and salicylates. “Therefore, these controlled challenge studies do not appear to have addressed adequately the role of diet in hyperactivity.” (See Defined Diets and Childhood Hyperactivity, published by the NIH in 1982).
1982 was years ago. Newer, better designed studies have shown a success rate between 58% and 81% depending upon the design of the study.
The Diet Connection
Most of the families who use the Feingold Program do so to help a child who has been diagnosed with ADHD. Researchers have found that children with ADHD frequently have additional health and behavior problems such as the symptoms we list elsewhere.
When Dr. Feingold first began to use diet (then called the K-P diet) to treat children with ADHD (then called hyperkinesis), he said that 30% to 50% of them got better. Later, after he also eliminated the petrochemical preservatives BHA and BHT (TBHQ didn’t exist yet), he found that over 70% of the children got better.
About 50% of children (or adults) don’t need any other intervention. The others still need more help, which may be educational adjustments, tutoring, supplements, further restrictions due to identified allergies, behavior modification or counseling, or some sort of medication including stimulants. While some people do use both the diet and stimulant medication, they appear able to use less medication than expected.
I have never seen any research done on this phenomenon, although one old study did point to it (Williams 1978). Using a computerized test of attention called the TOVA, I myself did an undergraduate independent study in college in 1998 which found a clue:
The TOVA reports 4 parameters, two of which are called “cognitive” and the other two are called “behavioral.” All four must be in the normal range for the child or adult to behave and learn normally. When used to monitor the effects of Ritalin on a child, the “cognitive” parameters rise to normal first, according to the TOVA company. Under increased medication, the other two rise.
However, I saw that when put on the Feingold diet, the “behavioral” parameters of each child rose to normal first, followed by the “cognitive” ones. If using both diet and Ritalin, theoretically, the diet would raise the “behavioral” parameters while the medication would raise the “cognitive” ones at the same time. Therefore, it makes perfect sense that less medication would be needed for the best effect.
Some Feingold members find that during high pollen seasons, their allergic children need more than the diet alone – some benefit from a very tiny dose of medication during that time. Unfortunately, no studies have been done on the relation of allergy to the need for medication, or why medication would be needed only during those times, but if this seems to be a problem in your family, work with your doctor to achieve the best possible results for yourself or your child.
Go to studies on ADHD